July 11, 2026
Why is Euthanasia Increasing in Netherlands?
Why is euthanasia increasing? Study points to aging population, assertive patients, and a healthcare system falling short’ by Christiaan Pelgrim.
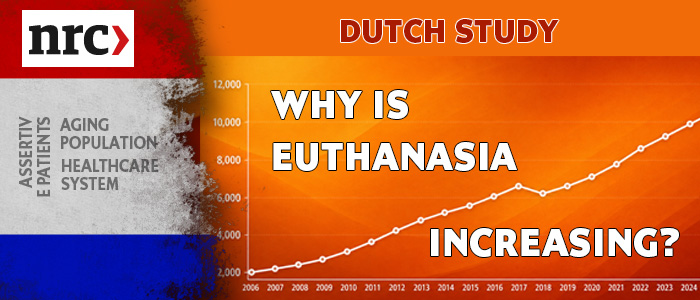
Over the past 25 years, the number of euthanasia cases in the Netherlands has risen sharply — from around 2,000 to roughly 10,000 per year.
In relative terms, euthanasia accounted for 1.6% of all deaths in 1999, rising to 5.8% in 2024.
At the request of the Dutch parliament, a large-scale study led by care ethicist Els van Wijngaarden (Radboudumc) examined the reasons behind this rise, drawing on scientific literature and interviews with practitioners.
Key Findings
Those involved in Dutch euthanasia practice mostly describe the increase as a “logical development,” driven partly by an aging population and a rise in cancer and chronic illness.
Cancer is involved in 54% of all euthanasia cases, though the fastest growth is now in other categories — combinations of conditions, dementia, an accumulation of age-related complaints, and psychological suffering.
Euthanasia has become more visible, discussable, and accessible for people with a wide range of diagnoses — something most practitioners view as a positive development.
Societal attitudes have also shifted, with people increasingly wanting control over their own life and death.
Healthcare shortcomings as a possible factor
The report doesn’t present healthcare system failures as a major, scientifically proven cause of the rise, but flags it as a serious signal worth taking seriously — since the euthanasia law can only function responsibly alongside accessible, good-quality care.
Specific concerns raised
Shortages in home-based terminal care sometimes mean people who want to die at home can’t get the care they need, making euthanasia a possible alternative.
Some elderly people see moving into a nursing home as a “nightmare scenario” to be avoided.
Mental healthcare (GGZ) is least accessible for patients with the most complex problems, who face long waitlists — potentially worsening the very suffering that leads to a euthanasia request.
Van Wijngaarden cautions against oversimplifying this: you can’t simply say “poor care equals more euthanasia.”
But she notes real concern, particularly in mental healthcare, that inadequate care may reinforce patients’ wish to die.
The researchers recommend that the Ministry of Health maintain accessibility and capacity in mental healthcare, elder care, and home-based terminal care, and further investigate how care shortages affect euthanasia requests.
Loss of dignity and changing tolerance for suffering
Practitioners report a declining societal tolerance for suffering.
“Unbearable suffering” — a legal requirement for euthanasia — used to be mostly associated with severe physical pain; now people also fear loss of dignity and future suffering.
Death is also becoming “medicalized”: one quoted GP describes doctors as first trying to prevent dying, and when that’s no longer possible, “getting rid of it” via euthanasia.
Some doctors report feeling pressured by patients and families who believe they’re entitled to euthanasia (“I have a right to it, don’t I?”), even though the law requires the doctor themselves to be convinced of unbearable and hopeless suffering.
The report warns against a situation where patient autonomy dominates — autonomy is just one of several core values under the euthanasia law, which must be weighed against the “protection-worthiness of human life” and related due-care requirements.
Van Wijngaarden stresses that vulnerable patients also have a right to protection: doctors shouldn’t give up on a patient too quickly, and a request made “in a moment of despair” shouldn’t be met with quick agreement.
Media are also cited as contributing to a one-sided or romanticized image of euthanasia as a “good death,” leaving alternative ways of dying underexposed.
Exit