November 6, 2016
Why America’s Medical Aid in Dying Acts are Failing Seniors
In recent weeks, the Dutch Ambassador to New Zealand, Robert Zaagman, has described NZ political debate about whether to introduce a voluntary euthanasia/ assisted suicide law as being akin to Dutch debate 20 years ago.
While an increasing number of US States are moving beyond the ‘should we’ – ‘shouldn’t we’ legislate on end of life choices, the model that States such as Colorado and Washington DC are envisaging is far from ideal. Indeed it could even be discriminatory and cruel.
In Exit’s opinion, the chosen model of law is so firmly predicated on the medical model of doctor-assistance that it disenfranchises the majority of older people who would seek control over their end of life.
Let’s explain:
On 8 November, Colorado – with its Proposition 106 – is expected to become the third State to pass a ballot to legalize ‘medical aid in dying’. (Colorado will follow Oregon and Washington).
Colorado will join Oregon, Washington, Vermont and California in legislating for end of life rights. (While Montana case law has confirmed the legality of assisted suicide, that State is yet to legislate).
Like all other States, the Colorado legislation is not only ridiculously restrictive but it places the control disproportionately in the hands of the doctors.
Take a look at the qualifying criteria.
1. The person must be an adult
The law refuses to acknowledge that teenagers (aged 18 years and under) can be unlucky enough to get terminal diseases.
Neuroblastoma, for example, is a common childhood cancer. Survival rates are 1 in 2. However, there is very little treatment if relapses are experienced.
Why should young people with this cancer not have the same rights to end their suffering as their adult counterparts. Especially given the advanced maturity of young people with terminal illness and the fact that they are already expected to make decisions about their various treatment options.
2. The person must be terminally ill, with six months or less to live
This type of so-called ‘safeguard’ is inherently problematic.
Firstly, many terminal illnesses do not have a defined timeline prognosis.
This means that some folk with a terminal illness will fail to qualify to qualify.
You can’t just have cancer if you want to be prescribed your lethal drugs. You must have really-advanced or really fast-moving Stage IV cancer.
Determination of a person’s prognosis sets physicians up as futurists, and as Gods.
This is neither logical nor fair. There is no crystal ball when it comes to being ill.
Secondly, and equally importantly, the criteria of six months or less to live excludes people with, for example, Multiple Schlerosis or other painful conditions such as Rheumatoid Arthritis.
And what about people with disabilities such as Tetraplegia who may live forever but who have had enough, but can’t help themselves to suicide?
Or what about eye conditions such as Macular Degeneration?
Over the past 20 years, Exit has been approached by many many older people with conditions such as these.
While they may not be our reasons for wanting choice in dying, they are some people’s. And they deserve respect.
Colorado’s law will exclude everyone but those who are ‘almost dead’ anyway.
3. The person must be mentally capable of making their own healthcare decisions
At law, capacity is a presumed fact. That is a person is considered to be capable of making decisions about any number of issues, until they are proven otherwise.
In medicine, however, it is a lack of capacity that is presumed.
This means that capacity to make decisions must be proven. And it must be proven without doubt before that person will be able to qualify to use a law such as that being proposed by Colorado.
In a real life scenario, this presumed lack of capacity means that the person wishing to be prescribed end of life drugs (so they have an option in place) must prove to two different doctors (one a psychiatrist/ psychologist) that they are of sound mind.
This means the very very sick person must subject themselves to even more medical testing. And what for? They are going to die. This is simply so they can die ‘well’.
If they are not able to prove they have capacity (for example if they are depressed), they will still be terminally ill. They will still be on the trajectory towards a premature death.
The only difference is that they will be deprived of their Nembutal.
Is this good enough? We don’t think so.
4. The person must be fully informed of all their options for care, including pain management, palliative care, hospice and comfort care
This requirement has been a standard feature of all laws in this area, and dates back to the Northern Territory’s Rights of the Terminally Ill Act of 1995.
In reality, this requirement means that the person must be spoken to – perhaps in a childlike fashion – to ensure that their decision to decline further (often miraculous but high intrusive) medical treatment is one made in full knowledge of such options.
5. Two physicians must determine the person has no mental condition impairing their ability to make decisions and is free from undue influence or coercion
There is always the rumor that granny is being encouraged to die so the greedy relatives can inherit her house, savings etc.
At Exit over the past 20 years we have seen extremely little evidence of this. We are not saying that ‘elder abuse’ does not exist, but that it is not common.
The requirement for two doctors to sign off on one’s sanity serves to ram home Medicine’s message that you are not thought to have capacity to make decisions about your life and death until you have proven to two doctors that you do.
6. The person must be able to take the medication themselves
The requirement that the person must take the medication themself is something that even Switzerland demands.
The purpose of this requirement is to ensure that the act is voluntary and that a third party is not forcing death upon a would-be victim.
It is a reasonable requirement but it does rule out those who are not able to move.
For example, where does it leave a person with a disease such as Lou Gehrig’s (ALS/ Motor Neurone Diseases) and another neurological illness: conditions that rob a person of movement?
Does this requirement mean that such people must take the medicine while they are still physically able?
Yes it does.
A right to die law that brings death forward in time is hardly a good thing.
This is a significant drawback of the law being proposed in Colorado and in play elsewhere.
7. The person must be a Colorado resident
Ahh death tourism.
Colorado is just fine with tourism based on their famous great outdoors, they are not fine with out-of-staters flying in to die.
What are they so afraid of?
Only Switzerland allows non-residents to use their enlightened assisted suicide law.
8. The physician must offer the person multiple opportunities to take back the request for aid in dying medication
First step to use the CO law is that the person must be terminally ill with less than six months to live.
As problematic as this is, the law also demands that the person’s request end of life drugs (so they have control over their life and death) is further tested.
For God’s sake. The person is about to die anyway!
What sort of Indian Giver offer is this?
This requirement assumes that the only reason the person is still alive is because they haven’t yet got the means to end it.
If we are talking about a totally rational adult in the most advanced stages of a terminal illness are we not talking about a person who wants to hang in there.
A person whose decision about their short future has been a long time coming and is extremely well considered?
This is a ridiculous ‘safeguard’ and is testimony to all that is wrong with the medical model of assisted dying.
9. Two witnesses must sign the request form confirming that the person is mentally capable and the request is voluntary
More red tape. Remember we are talking here about a person who is about to die. It is not as if the person who is terminally ill with less than six months to live is about to miraculously get better.
Surely bureaucracy should be kept to a minimum?
Two witnesses? ‘Whatever’ the dying person will say. If they can muster the energy and enthusiasm.
10. Wills, contracts, insurance and annuity policies are not affected by a person choosing aid in dying
Guarding against discrimination is an important goal. Ensuring one’s life insurance policies will not be affected, simply because one is electing to go a few months, weeks or days early is a good thing.
Summary
The model of law reform being voted upon by Colorado pure medical model on issues of power and control.
The patient must perform to the satisfaction of the physicians present. The doctors will decide who gets help (and dies ‘with dignity’) and who dies with no help and even less dignity (or even violently as that is all they can do).
The Colorado law provides no scope for those wanting the peace of mind that comes from knowing that one has lethal drugs locked away in the cupboard, just in case.
This is not a law that serves the vast majority of older folk who wish to have control over when and how they die.
The Colorado law is a law of last resort for those who will die in the very near future.
If these people are considered those most in need, then the law is a good thing.
It is directing resources to those who need them most.
But if end of life rights are considered more broadly, Colorado and California and Oregon and Washington and Vermont are all failures.
Under all these legal models, medical aid in dying is – as its name suggests – a medical treatment
None of these laws serve the vast majority of the over 70s.
None of the laws bring any benefit to those who are not ill (now) but who wish to be prepared for the contingencies of the future.
Dying well – euthanasia – is not yet a civil right.
Is this reason not to support such ballots? Likely not. But beware.
As Law Professor Susan Stefan – author of Rational Suicide Irrational Laws (Oxford University Press 2016) has argued, ‘once you let doctors into our lives (and deaths) you will never be able to get them out!’
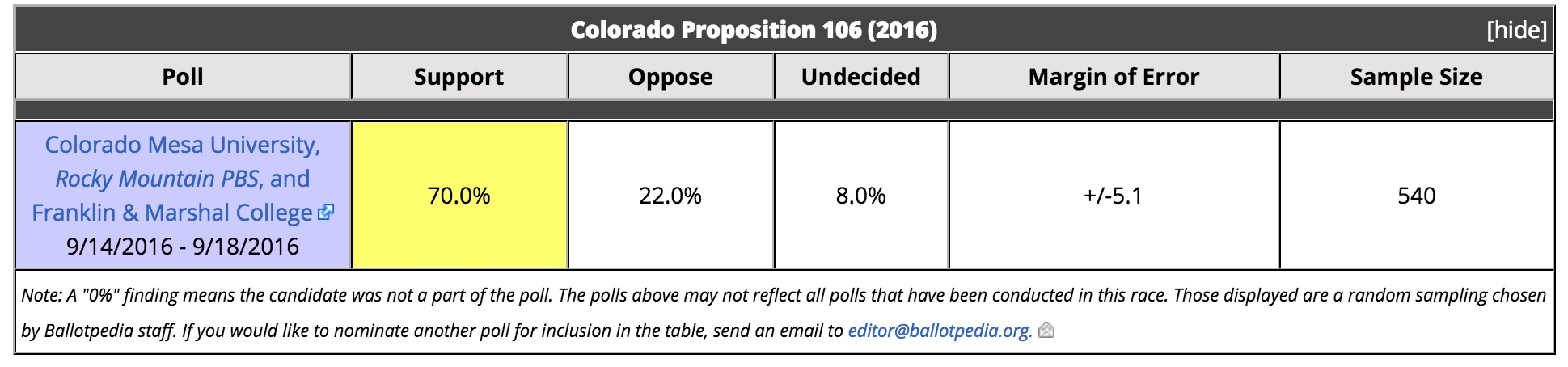
Colorado Poll showing 70% support
The Dutch Direction
In the past month, the Dutch Government has announced that by 2018 it will legislate for older people who feel they have ‘completed life‘ to get help to die.
While the medical profession will still be the gate-keepers, the Dutch plans are a first step towards treating the good death as a civil right for all citizens.
All older citizens of sound mind regardless of their physical health will be able to request medical help to die.
Perhaps we should be asking the Dutch Ambassador to the US, Henne Schuwer, if the debate that Colorado and Washington DC are now having about end of life rights is what the Dutch had 10 years ago.
Would be interesting to see his reply.
Citation Requirements
To cite this article, please include reference to the author, the title, the date of publication & the citation link below:
https://www.peacefulpillhandbook.com/?p=2480
Browse the Peaceful Pill eHandbook
Exit